
What Even Is a Normal Period in perimenopause Anyway?
- lauriealpertnd2
- 4 days ago
- 6 min read
She'd had the same cycle for twenty years. Every 28 days, like clockwork. A few days of cramps, some PMS she could set her calendar by, and then it was over. Annoying, but predictable. Manageable.
Then, somewhere around 44, things shifted. Her period showed up nine days early. Then it was two weeks late. One month it was so light she almost missed it. The next, she went through everything she had in her bag before noon and nearly cancelled a work presentation. She Googled "irregular periods 44" and fell down a rabbit hole of forum posts, contradictory headlines, and supplement ads.
By the end of it, she had seventeen tabs open and still no real answer to the question she'd actually come with:
Is this normal?
If this sounds familiar, you're in the right place.
First, a quick note before we talk period
Cycle changes are often the most visible sign that perimenopause has officially begun. But for many people, the hormonal variability of this transition shows up in other ways first: sleep disruptions, mood changes, brain fog, sometimes years before a period does anything unusual.
And here's something worth calling out clearly: not everything you're feeling is hormonal. Perimenopause is having a moment right now, and it's easy to assume that every mood swing, every disrupted night, every memory lapse, every symptom in midlife is the result of shifting hormones. Sometimes it is. Sometimes it isn't. Thyroid changes, iron deficiency, mood disorders, sleep conditions, and other factors can produce very similar experiences, and they require very different responses. This is one of the most important reasons to work with an informed provider rather than self-diagnosing from a podcast: you need a critical eye that can help you discern what's actually driving what, especially when your cycle hasn't changed at all.
If any of those things are bothering you, that's worth a conversation with your healthcare provider, independent of what your cycle is doing. You don't have to wait for a "sign" to ask for support.
Okay. Now let's talk about periods.
What does a "normal" cycle actually look like
Before we get into what changes, it helps to have a baseline.
A typical menstrual cycle runs anywhere from 21 to 35 days, measured from the first day of one period to the first day of the next. That's a lot more variability than most of us were raised to believe. Bleeding usually lasts 2 to 7 days. There's a lot of variation within that range that still counts as normal. People have shorter cycles, longer cycles, heavier days and lighter days, and none of that is automatically a problem.
What matters most is your normal, the rhythm your body has established over time, and whether that rhythm is changing.
What actually changes in perimenopause, and why
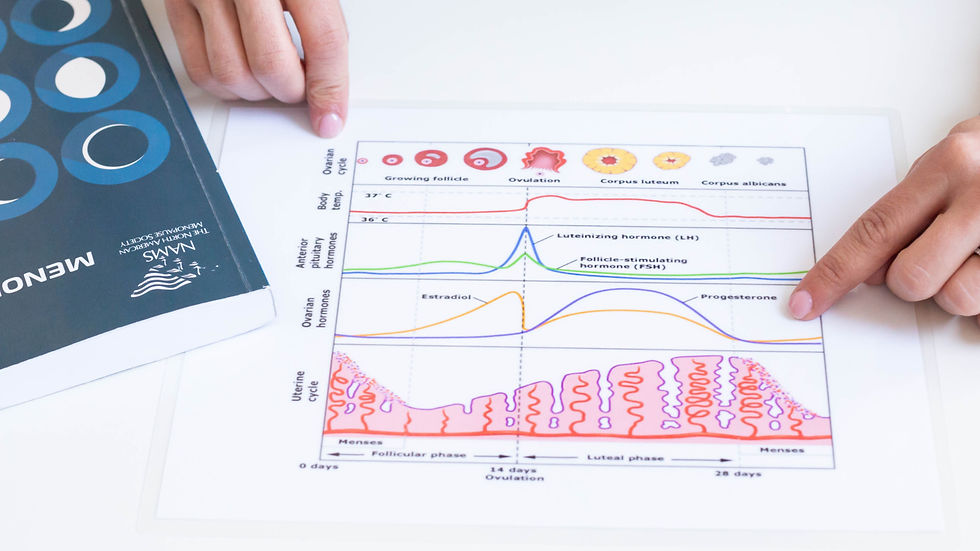
Perimenopause is not only a hormonal experience. It's a whole-body transition, one where multiple systems are affected by changes in hormonal production by the ovaries and the communication between your brain and your ovaries. Ovulation becomes less predictable. Estrogen levels fluctuate, sometimes dramatically, rather than following their usual rhythm. Progesterone, which is often the first to decline, drops off when ovulation doesn't happen.
All of that shows up clearly as changes in your menstrual cycle.
Here's what's genuinely normal, meaning variable but not automatically concerning:
Cycle length changes. Cycles that were reliably 28 days may become 24 days, or 35 days, or something in between. Some months may be a little longer, some a little shorter. This variability is one of the earliest and most consistent signs of perimenopause in someone over 45 with no other concerns. In someone younger than 45, this kind of variability warrants a thorough look and assessment before assuming early perimenopause is the cause.
Flow changes. Lighter periods are common as estrogen declines. But heavier, longer, or more intense periods are also common, particularly in early perimenopause, when estrogen can fluctuate to even higher-than-usual levels before it begins its overall decline. Irregular bursts and spurts of ovarian hormones throughout this transition are why your period can suddenly feel so unpredictable and all over the place.
Skipped periods. Missing a cycle, or several, becomes more common as you move further into perimenopause. Technically, menopause is defined as 12 consecutive months without a period as a result of ovarian function decline. That distinction matters: many people don't have regular periods because of an IUD, continuous hormonal contraception, or other factors, and that's a different situation entirely. If you're in that category, the conversation about where you are in this transition looks a bit different, and it's worth having directly with your provider.
Spotting between periods. Small amounts of bleeding or spotting between cycles can happen as a result of the hormonal fluctuations of this transition. It's worth noting when it happens so you can tell your doctor clearly, more on that below.
Worsening or shifting premenstrual experiences. Some people find their premenstrual experiences intensify during perimenopause: more irritability, more fatigue, more difficulty with mood in the days before a period. This isn't always a diagnosable condition, but it's real, it's common, and it's worth naming. Perimenopause can also significantly worsen pre-existing premenstrual conditions. If your premenstrual window has started to feel like a different person takes over your life, that deserves your attention, not denial or acceptance.
What's worth tracking
You don't need an elaborate system. The single most useful data point is the first day of each bleed. Jot it down somewhere, consistently. That information tells you how long your cycles are running, whether they're getting shorter or longer, and gives your provider something concrete to work with.
Beyond that, pay attention to:
Whether spotting is happening between periods, and when
Whether the character of your flow is changing: significantly heavier, significantly lighter, or lasting noticeably longer than it used to
Whether you're passing clots larger than about a quarter
Whether bleeding is interfering with your daily life in any way
My free Perimenopause Primer offers a tool to help you keep track of all of this.
When to talk to your provider
Here's the honest answer: if it's bothering you, it's worth a conversation. That's not a low bar. That's the actual clinical bar. Heavy bleeding is thankfully no longer defined by millilitres or a specific number of products used. It's ultimately defined by impact. If your period is affecting your quality of life, your plans, your sleep, your work, your sense of yourself, that is clinically meaningful, and you deserve support.
Beyond quality of life, there are specific changes that warrant a conversation regardless of how you feel about them:
Bleeding that soaks through a pad or tampon in 2 hours or less, more than once in a row.
Clots larger than a quarter
Bleeding that lasts longer than 7 days, including spotting
Spotting or bleeding between periods, particularly if it's new, recurring, or unexplained
⚠️ Any bleeding after 12 consecutive months without a period. This is postmenopausal bleeding, and it ALWAYS requires evaluation. Even if it seems minor, even if it was just a little, even if you feel completely fine. This is one that many people don't know about, and it matters. Please don't wait on this one.
Cycles that become very short (less than 21 days) consistently
A sudden, significant change in your cycle after a long period of stability
These changes don't always mean something serious is happening. But they can be caused by things entirely separate from perimenopause: fibroids, polyps, thyroid changes, and other conditions that are worth ruling out or addressing. A provider who knows your history can help you figure out what's actually driving what.
The question under the question
When someone asks "is this normal?" about their cycle, what they're usually really asking is: Is something wrong with me? Am I going to be okay? Does anyone understand what I'm going through?
The honest answers: probably not, yes, and absolutely.
Perimenopause is not a crisis even if it can sometimes feel like one. It's a transition, a significant one, with real experiences that deserve real attention. Most of what you're going through is the predictable result of a body doing exactly what it was designed to do at this stage of life. That doesn't mean you have to white-knuckle through it.
If you're ready to stop guessing and start understanding
If you're in the thick of cycle changes and you want to understand what's actually happening in your body, and what, if anything, to do about it, I'd love to be part of that conversation.
One-on-one care is designed for exactly this. This can include ordering and reviewing bloodwork together or helping you understand results you've already been given, whether you were told everything looks "normal" or you've been offered a treatment you're not sure about yet. When imaging or other investigations are needed, I'll help you understand when it's time to loop in your doctor, and work respectfully with your other care providers to help you get the care you need. The goal isn't to replace your existing care. It's to make sure you're not navigating it alone, and that you actually understand your options well enough to make decisions you feel good about.
If that sounds like what you've been looking for, you can learn more about working with me or book a discovery call. You don't have to figure this out from 17 (or more!) browser tabs by yourself.
Dr. Laurie Alpert is a Naturopathic Doctor and Menopause Society Certified Practitioner specializing in perimenopause and midlife hormonal health.


Comments